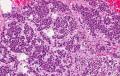
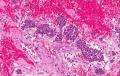
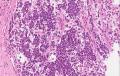
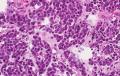
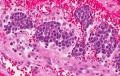
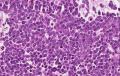
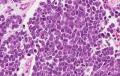
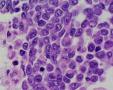
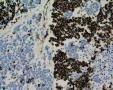
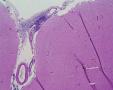
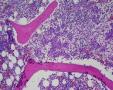
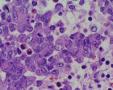
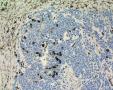
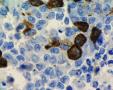
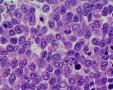
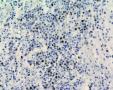
3 years girl was hospitalized due to lower limb paresis. on CT scan small tumor nidus was found in retroperitioneal left lumbar area with spread to spindal cord, mts to the cerebral meninges. The patient was deceased soon due to difusse cerebromalacia/liquor drainage blockage. Autopsy shows the same tumoral spread (difficult visualisation due to small mass), prominent neuro- tropism and distant mts to bone marrow and CNS coverings.
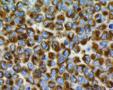
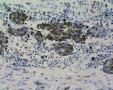
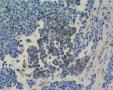
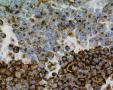
Clinically and at first glance histologically the idea of neuroblastoma possibility was evolved. Any clinical/molecular/biochemic analyses regarding neuroblastoma version were done due to rapid course of the disease. Immunophenotype: Vimentin+ 20%; PanCK+ 10%, Cam 5.2+ 5%; NB84+ 60%; EMA+ 70%; ChromograninA/Synaptophysin(-); S100+ 10%; Desmin/MyoD1 (-), CD99(-)(single focus <5%+), CD56(-), NSE+ 10% (patchy), CD68/MelanA/HMB45(-), Hepa/CD57/CD34/NFP/GFAP(-), CyclinD1(-), CD20/CD30/CD3/LCA(-); p53+ 10%. Ki67 prolif. activity ~40%. PROPOSAL: Small blue round cell tumor with rhabdoid features, maybe extrarenal rhabdoid tumor (paraspinal) vs epithelioid MPNST (exceptional in this age group) with spread to spinal cord and mts.
Gallery:
Annotations
»
Add comment
(Login)
|
























Last modified: 2011-07-05 10:42:40