
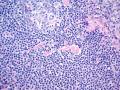
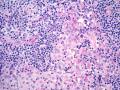
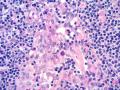
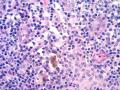
We present here a new case of the the enlarged inguinal lymph node, extirpated in a 24-year-old Bosnian male.
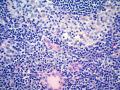
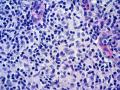
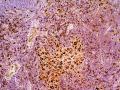
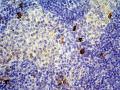
He was admitted to the Department of Infectious Diseases due to the fever and enlarged, painful inguinal lymphadenopathy follow by malaise and weight loss. WBC: Anemia and neutrophilia; CRP 184;Increased Alpha2 and Gamma globulins. Clinical examination revealed also hepatosplenomegaly and right axillary lymphadenopathy confirmed by ultrasonography. CT scan showed retroperitoneal lymphadenopathy. Microbiology: Negative for Toxoplasma, Cytomegalovirus, Herpes simplex, EBV, Mycoplasma pneumoniae, Brucella sp., Coxiella Burnetii. Serial analysis of his stool revealed no pathogenic microorganisms. He has been treated with antibiotics but without effective results. An inguinal lymph node, that measured 2.8x1.5x0.8 cm was received for histopathological examination. Histopathological examination showed generally preserved the structure of the lymph node. It also revaled dilated sinuses with histiocytes, lymphocytes and plasma cells. Focally, in subcortical areas sporadic histiocytes, lymphocytes, plasma cells and eosinophyls were noticed. In interfollicular areas some plasma cells and eosinophils were seen. Immunohistochemistry: CD1a(+), S100(+), CD68(+), CD3(-), CD20(-), CD30(-). Clinical diagnosis: No Histopathological diagnosis: Reactive lymph node? Please, give your opinions. anotacija
»
pridėti komentarą
(prisijungti)
|








Last modified: 2007-12-05 19:36:13