
HISTORY: 79 yrs old female with uncertain diagnosis: 2 previous skin biopsies reveal granulomatous process, most probable "actinic granulomatous" (2007 August- September). Clin.: purple nodules and plagues on the face.
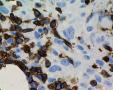
Threpine biopsy: low quality, most probable reactive changes (no photographs). Lymph node biopsy was taken in November due to "disseminated lymphadenopathy": due to my "sympathy" to granulomatous processes the general IH panel was applied to this "sarcoid" like lymphadenitis with clusters of large cells with polylobated nuclei with a huge nucleoli in sinus and paracortical area, vague nodularity/septation: CD30+ CD43+ CD15- EMA- CD20- CD3- Bcl6-. GranzymB/ALK1/CD4/CD8/EBV LMP1 negative. The admixture of plasmacytes are present. PROPOSAL: cHL unclassified (probable NS 1?) with prominent granulomatous/sarcoid like reaction in LN. WORKING DIAGNOSIS: T lymphoma in the skin with the prominent granulomatous reaction and spread to LN. Thank you for participation.
galerija:
anotacija
»
pridėti komentarą
(prisijungti)
|


























































Last modified: 2007-12-10 10:38:07