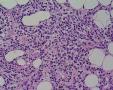
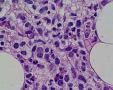
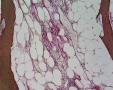
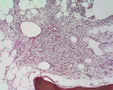
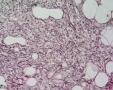
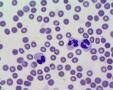
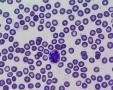
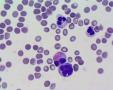
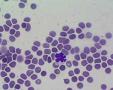
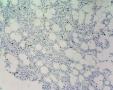
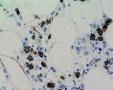
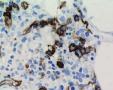
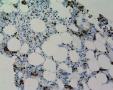
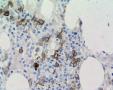
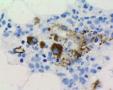
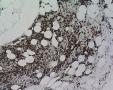
55 yrs male with threpine biopsy and aspirate.
Diagnosis: aplastic anemia. History: 1 day patient from foreign country is under evaluation for BM transplant. Threpine hypocellular with fibrosis, arhitectural distortion, lymphoid agregattes and Fe deposition (MDS like picture). Only single micromegakaryocytes. Scattered NASDE+ granulopoietic cells, single erythroid cells, multiple eosinophils, maybe mastocytes are present. Some NASDE(-) precursor cells with "blastic" morphology. Blood test is attached. Smear: Photos are made with standard 60x lens. In case I have 100x oil in reserve:) An aspirate seems to be low cellular, foccaly overcrowded by erythrocytes. IH (hot spots): CD34/CD117+ precursors with slight clustering up to 20%; CD117+ mastocytes; Lymphos: CD3+ >> CD20+ (single); Single CD138+ plasmacytes; CD34+ neovascularity is prominent. vWF+ single micromegakaryocytes. WORKING: Architectural distortion with excess CD34+/CD17+ precursors up to 20% (scant hematopoietic population at all), III-IV fibrosis and prominent Fe deposition: high grade MDS is suspected. The use of CSF must be excluded. Please comment all diagnostic things, especially techno aspects and cytology. Thank you a lot.
Gallery:
Annotations
»
Add comment
(Login)
|












Last modified: 2008-11-06 09:40:22